Transcript
Charles Runels: Thank you guys for attending. I hope that I can really bring to you something that will change your life. I was just chatting, and I just realized I hadn’t started the thing. I promise you I’m a better doctor than I’m a webmaster.
Charles Runels: Here’s the purpose of this. Basically, I think that female orgasm and female sexuality has not been talked about enough. It hasn’t been researched enough, and because of that, women have suffered a long time without the help they need. There’s over 20 drugs and devices to help men with their sexuality. We have one drug to help women with their sex now, and it’s a side drug. We’re far behind, I think, and sexuality also has this odd thing about it in that it’s like a psychological disease in that people feel embarrassed when they have it.
Charles Runels: For example, if you had, to help explain what I mean by that, if you had a broken arm or you had breast cancer, you would probably tell your friends about it and ask them to think about you or pray for you or at least give you whatever support, but if you have schizophrenia or major depression, maybe you keep it a secret because we still have this ideal that psychological disease is embarrassing and that we shouldn’t even talk about it, but it has a physiological basis. Bipolar disease or schizophrenia or major depression has true biochemical basis for it, and there’s really no reason why we should be embarrassed by it, but, still, people are ridiculed, and they get very little sympathy. If you’re, say, you’re majorly depressed and your life looks great from the outside, your friends may not give you much sympathy, and to prove my point, just go on the blogs and look where people post about sexual dysfunction. You’ll see flippant remarks, like, “Well, you just need a lover with a Gold or Black American Express card,” or they just need to spend more time with foreplay, just flippant remarks when, try to say that to a women who has Lichen sclerosus or painful intercourse because she delivered a large baby.
Charles Runels: We have this idea, I think many people do, that women should be able to heal themselves when they’re depressed or think panic attack. Well, just get a grip. Why are you panicking? Well, they’re panicking. Panic attacks happen because major things go on with brain chemistry, and you can no more think you’re way out of it than you can think your way out of a melanoma or basal cell carcinoma.
Charles Runels: It’s really bothered me that after taking care of thousands of women, there’s still a lot of that that goes on. You can see that by looking at things like look to see what happened when flibanserin was presented to the FDA. There was a large group of sex therapists who showed up to protest the approval of that drug, and with the implied and sometimes non-implied idea that counseling can take care of everything or just sensate focus and all the things we do, all of which is important, but doesn’t make everything better.
Charles Runels: Here’s what I think is needed. When you’re thinking about individual parts, sometimes it works, if you happen to catch the person that that’s the thing they need, but, oftentimes, it doesn’t work because there’s something else broken and because people aren’t thinking in terms of systems, systems. We do that with other things, like the respiratory system, and we know that, for example, if someone’s short of breath that perhaps a bronchodilator won’t help them if they’re short of breath and their problem is, let’s say, a foreign body in the left mainstream bronchus, so that they can’t even get something back and forth because they aspirated a toy, and it’s a child, for example, or they’re short of breath because they’re profoundly anemic and their lungs are working fine, but they don’t have enough blood cells to carry the oxygen.
Charles Runels: The respiratory system, the reason we think in terms of systems analysis is to keep from thinking that everything is the proverbial nail because we have a hammer and that hammer might be surgery if you’re a gynecologist, it might be therapy if you’re a sex counselor, it might be an O-Shot if you’re me, who invented the O-Shot. To keep that from happening in the rest of medicine, we have systems, and we think in terms of systems, how all the parts work together. It seems odd to have to defend this idea, but because it’s so ubiquitous than other parts of the body, for example, the gastrointestinal system, the cardiovascular system, and you can just look, if you Google, if you just put in here respiratory system into your Google search bar, you already know what it’s going to show from your sixth grade chemistry or sixth grade biology class, umpteen pictures of the respiratory system and how it works, everything from how the air travels down, to how the oxygen exchanges in the alveoli and gets into the bloodstream, and then the carbon dioxide comes out, the whole thing, lots of diagrams about, here, there’s the circulatory system, how oxygen is moved then through the bloodstream so that oxygen can be delivered and carbon dioxide removed.
Charles Runels: I think that it would be helpful if we had something like this, an atlas or a chart, so that when we think in terms of the orgasm system, not the reproductive system … There’s a reproductive system, and I think because we have … Here’s the female reproductive system. Because we have these ideas so commonly thought about and everybody learns to draw this picture somewhere in high school, maybe we take the systems analysis concept for granted, but it’s really important to understand both how things might not be working and how to make them work better, whether it’s making normal better or making abnormal well. That’s the idea behind this. It’s not complicated, but it’s not simple, either. It’s not just here’s the clitoris, and that’s the orgasm system. Much, more more elegant than that.
Charles Runels: The way I’ve divided this up and thinking about the … Oh, a little bit more, before I get to how I’ve divided this system up, because you have to think, are you going to divide anatomically, physiologically, metabolically? How will you divide it up? Well, if you look what’s normally done, the systems are a group of parts, and it’s usually described in physical anatomy, things that you could look at on dissection or you could palpate or look at if you’re standing in the room with someone. Then, the physiology and the biochemistry and the pathology is then thought about in terms of those anatomical parts. That’s how I think we would think about this.
Charles Runels: The goal is that actually that I’m grateful for you guys for getting on the call because I’m going to present to you what I’ve worked on so far to create a simple chart with an explanatory book, and then your feedback to me will be great because it will help me edit it, and then I’ll take what we do here, and, your feedback, it’s like you’re helping me edit the book before it’s put out. Then, I’ll produce the book, and I’ll send you a copy for free that’s signed with my many thanks for helping me do this. You’re helping me edit a book that I’ve already written about the female orgasm system.
Charles Runels: I was talking earlier about how I’ve taken care of thousands of women. I’ve invented, in doing their hormones and thinking about their sexuality, I invented the O-Shot as part of a way to fill in the gaps where hormones won’t do or for women who can’t be on hormones, and then now have trained literally thousands of doctors in 50-something countries, and we have doctors training for us, and all that really doesn’t mean jack because what really matters is when one person is sitting in front of me in my office. Do I have a way of thinking about them in an organized manner and to getting to a way to make them well? To me, I feel like we’re still failing as physicians when we have 30-40%, depending on how you read the statistics, of women who have sexual dysfunction defined in the strictest way, which means psychologically distressed because their sexuality is working in a way that’s not pleasing and literally disrupting their life in some way.
Charles Runels: Let’s think about the different parts that I, anatomical parts, that I would think about, and then I thought I’d cover the first part of that, which is the brain, on this call, and we’ll just do a chapter a week with your feedback about what else you would like to know at the end, and I’ll answer those questions for you, and that’ll become part of the book.
Charles Runels: The way I would think about the orgasm system for a female is in terms of the brain, and the brain has mid-brain, the cerebral hemisphere, and I think the pituitary gland has to be thought of as part of the brain. Then the circulation, the breasts, and I would group together the remainder of the body, like hands and thighs, in a group. It’s less important. You could have good sex without one of your fingers, but still have something to do with sexuality. Then the nervous system or the spinal cord and then the clitoral-urethral complex, which includes the urethra, the corpus cavernosum, the pelvic floor, the muscles thereof, and the anus. That’s how I want to think about that and then how each part, each one of those anatomical parts functions to help with the orgasm system.
Charles Runels: One other quick analogy, and then let’s talk about the brain. Imagine that you have someone who’s trying to start a fire, but they are from some primitive age. They’ve never seen a fire, and someone tells them to have a fire, you really need a stack of wood, and they make a big stack of wood. That’s all they do, no fire. Then, they ask someone else, “How do you start a fire?” Someone says, “Oh, you need to light a match.” Well, they strike a match and throw it down, and the match goes out, not much happens. To really get a fire going, of course, they need to have someone say, “Well, to have a nice fire, what you really need is a stack of wood and then you put some lighter fluid on it, and then maybe you have some kindling underneath it to help it get started, and then you light your match, and then it takes off.”
Charles Runels: Sexuality is much more complicated than starting a fire. Yet, I think that what we see is that people have … They have the one thing that they push as the way to make this very complicated thing happen when what we really need is to think about all the ingredients. That’s enough about that.
Charles Runels: I hope that you find this useful. It’s not going to be long. My intention is that it be not the way you look and you find the answer to every problem. That would literally involve textbooks of gynecology. For example, with dyspareunia, there are so many things. There’s surgical things, there’s cysts on the ovaries, and how you would treat that. You could go so deep that you’d need literal volumes of textbooks to explain everything, but what I can do is outline it in such a way that all of the different parts are in front of us just like they are with the orgasms, with the reproductive system and the circulatory system and respiratory system, and the gastrointestinal system, and then thinking about all the parts together, hopefully, what will happen is you can use that if you’re a physician or a counselor or whatever, if you’re taking care of women and trying to have better sex, you can use that both as a way to structure your thoughts, just like you would if you were trying to get someone’s gastrointestinal system to work better, and you could also use it as hopefully a teaching aid to help people understand why there really are no magic bullets. We have to think about all the different parts and how they work together. If we can have a system for digesting your corn dog, we can have a system for understanding the depths of orgasm.
Charles Runels: Before we get to the brain, and I want to go through the cerebellum, the mid-brain, and the pituitary and how they work together to help with orgasm, before we get to that, I just wanted to say one quick thing about the importance of orgasm. Obviously, we can live very, very productive and fulfilling lives without sex at all. We can have productive and fulfilling lives and fulfilling sex lives without orgasm, but there’s something magic that happens with orgasm that goes on with the brain, that has really beyond explanation yet, but our observations are that people bond with what they’re thinking about, looking at, or interacting with when they have an orgasm.
Charles Runels: There’s actually a study where they looked at what happens with heterosexual men when they’re trapped in the Navy on a ship for a long time, and after turning to other men for their sexual release and being on the ship for a long time, heterosexual men become homosexual and start to seek a gay lover when … because they’ve learned to associate their pleasure with that. There is a bonding that happens, a deep psychological bonding that can happen with orgasm that lovers seek. It’s a legitimate thing to seek. If you can study this chart about the digestive system to seek a good bowel movement, it’s certainly worthy to think about orgasms and the orgasm system to seek that bonding. There’s also a psychological thing that happens where women especially will find they can be either energized or calmed down or become more creative. Sexuality [inaudible] and letters to a young poet talks about sexuality being related to creativity. They’ve talked about sexuality and sexual energy being related, just the ability to be a good businessperson in his book Think And Grow Rich, Napoleon Hill talks about sexual energy being related to the ability to make money and to be a good salesperson. Sigmund Freud even wrote an essay about how he thought that Leonardo Da Vinci was transmitting his sexual energy into creativity.
Charles Runels: There’s much more to orgasm than just the pleasure of the orgasm. There’s a psychological component. There’s a creativity. There’s a sociological and psychological bonding. There is much more than just a few moments of pleasure. It’s a worthy pursuit, and I’m glad to have you recognize that and go on this journey to help me define it and help me understand what I don’t say that you need to hear that I’m leaving off.
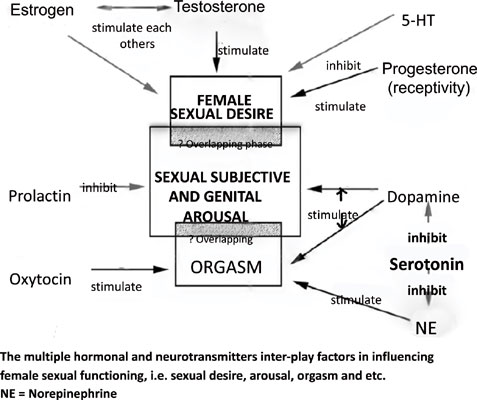
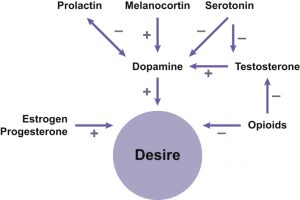
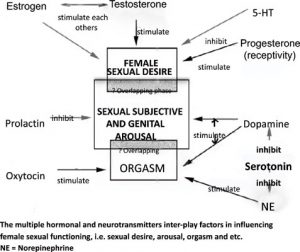
Charles Runels: Let’s talk about the brain one part at a time. Brain. You’ve got the cerebral hemisphere. You have the midbrain. Then you have the pituitary gland. Then you have certain neurotransmitters especially serotonin and dopamine. The new drug that is out has to do with modulating the ratio of serotonin and dopamine. Many people who are on Prozac, for example, have trouble with orgasm because of what happens with this ratio. Although their depression gets better, this ratio is off. Flibanserin changes the ratio in such a way that there’s an increase in libido. It’s not a lot. Average is about one extra encounter per month, and it’s not approved to help orgasm but libido goes up. These neurotransmitters are important. We’ll come back to that. Let’s just lay out some of the other things that go on.
Charles Runels: Cerebral hemisphere. There is a memory and a processing of what’s going on, so the situation. Now here’s the thing that’s different. Everybody was taught this thing about how there’s arousal and a plateau and then an orgasm and then resolution. What really happens with women, more so we think than men, is that women have a sexual encounter. If it’s unpleasant, then the next time they’re with a lover, especially that same lover, then it’s harder to become aroused. Then if that’s pleasant, it becomes harder to become aroused, and there becomes this negative spiral. After multiple negative encounters, it’s very difficult to have arousal or orgasm.
Charles Runels: On the other hand, this has to do with memory and situational interpretation with what’s going on. One of the reasons I like husbands to not be in the room or not be looking at their wife’s face when I do something that might be painful is I do not want the lover to associate pain with their lover’s face. There’s this memory and association. We all know it from having a smell or we hear a song that we remember having a sexual encounter with, and there’s an instant feeling of warmth and arousal that happens with that. There can be a negative spiral and a positive spiral.
Charles Runels: If a woman has an encounter that’s positive, it becomes easier for her to become aroused on the next encounter. Then even easier so that she can then be with that lover and even have an orgasm by that lover just speaking to her because she’s become so conditioned to associate the voice and that person with pleasure. Very, very possible for that to happen. Of course, a negative encounter can take it back the other way. Memory’s important. Situation’s important. Now how can these be affected? These two together, there was one study showing that if a woman does aerobic exercise for one hour post exercise, her ability to have orgasm is improved. Probably what’s happening is the same thing that happens when a woman has attention deficit disorder.
Charles Runels: If a woman or a man has attention deficit disorder, research shows that after aerobic exercise for the first hour or two, the person is better able to focus because of what happens with the neurotransmitters in the brain. We also know that the same medicines that help with attention deficit disorder can help a woman be able to orgasm. It’s a little difficult because those medicines are controlled substances. It’s difficult perhaps for your doctor to prescribe Adderall, for example, just for you to take prior to sex. But there are situations, there is some research backing up the idea that a low dose of Adderall prior to sex can make it more easy to have an orgasm. The closest you can get to that is if you get some of the diet supplements that are over the counter at Walmart that act similar in their effects on the parasympathetic and sympathetic nervous system, that that can actually work similar to Adderall.
Charles Runels: Now of course if you’re going to have sex in the evening, not such a good idea because it can keep you awake at night, but for the lunchtime or the morning sex, it’s a way to take what I just described to you and use it to increase the ability to have orgasm. Either having an aerobic … It doesn’t seem to work as well for resistance training. Nothing against lifting weights, but for orgasm, aerobic exercise seems to help more.
Charles Runels: Now what about alcohol? Alcohol or ethanol, it decreases the inhibitory systems so people are more likely to get naked, but in most women, it actually inhibits the ability to have an orgasm. I didn’t say it cuts it off. There are many women who have wonderful orgasms right after drinking alcohol. But the research shows that it can interfere with it while cannabis or marijuana can actually increase the ability to have an orgasm. Many women find that that first orgasm can happen after smoking pot or however you do your marijuana. I don’t do alcohol at all. I’m a teetotaler. I don’t smoke pot. But I do think that it has medicinal uses, and I think this can be a use for a woman who’s having difficulty having orgasm, learning to have an orgasm, can be facilitated with everything I just described to you. I would avoid ethanol. I think pot can help. I think aerobic exercise can help, and avoiding these negative encounters because that can really kill everything.
Charles Runels: Flibanserin is possible, but the problem with it is it still has that disclaimer that if you drink alcohol, you could die. The doctor, the pharmacist, and the patient all have to sign a thing that says that they know that. It’s kind of a buzzkill for a lot of people. But it’s a decent drug maybe worth trying. The other thing is if you do need to be on an antidepressant, obviously don’t stop it on your own. Everything I’m telling you here should be checked out with your physician. This is educational. I’m not your doctor. Obviously I haven’t examined you. I don’t know your situation. So I’m giving you things to think about and talk about with your doctor.
Charles Runels: But my favorite antidepressant is Wellbutrin (bupropion). This drug can actually help depression and facilitate orgasm and libido. There can be a transfer, so someone’s on say for example, they’re on one of the serotonin dopamine inhibitors, you could them … Say they’re on Prozac, you could wean them off of the Prozac and onto Wellbutrin and often their sex will improve dramatically just from that. Also, many women I have found who are being treated for depression, if you just treat their low testosterone, that will also help them with their depression and oftentimes they wind up not needing the antidepressant.
Charles Runels: Let’s talk about the pituitary gland. Pituitary gland, if you look at where it sits, it’s actually part of the brain. If this is the brain and right here is the pituitary gland. Actually if you operate on it, you can go through the nose to get to it. It’s sitting right there. It hangs down like a little pear from the brain. It’s actually part of the brain, and it’s part of the reason why emotions can affect the whole body. For example, if you get excited, a chemical is released. It goes to your adrenal glands. It causes the adrenals to release adrenaline and your heart rate goes up. This is probably a large connection between how thoughts and emotions can affect our physiology and cause disease or improve health.
Charles Runels: The thing is that although we know … I’m about to list some of the hormones that are produced by the pituitary gland, which is basically part of the brain, and how they can be manipulated either with pharmaceuticals or by behavioral changes. I’m going to go through some of these, but the pituitary releases over 200 hormones. Even though I’ll go into fair review of these, we have no idea really how those 200 plus hormones affect physiology. But the good news is that if you can correct the main things I’m telling you because one affects the other, people just get better without understanding all of it. Hopefully our understanding will improve. We will know more about how to fine tune things.
Charles Runels: Let’s plunge into some of these hormones. It’s kind of getting a little busy. Let’s do another. Here’s pituitary gland. Let’s start with one of the fun ones. It releases oxytocin which some people consider to be the love hormone. It’s released in just lots, just gushes out when a woman delivers. It causes uterine contraction and feelings of love for the baby she just delivered. Well, think about that. Uterine contraction and feelings of love, that could also be helpful in the bedroom. Some people have used this as an aid for sex because it’s a peptide chain. Think about what a peptide chain is. Think of a chain of amino acids. You got leucine and lysine and glycine, all these different amino acids that are in a protein that you eat. Then when you eat a hamburger or a piece of fish, your digestive system breaks the proteins or the amino acids down. Then your body reassembles them into a specific order that acts like a code or a word.
Charles Runels: Oxytocin is a peptide chain that has a very specific order of individual amino acids. The reason you can’t take it by mouth, insulin is the same way by the way, and the reason there’s no insulin pill is because if you take an insulin pill, your digestive system breaks it up just like it was a hamburger. Now these individual letters, metaphorically, have been scrambled and insulin is no longer insulin. It’s just digested protein. Oxytocin is like that which is why you can’t take it as a pill. It has to be either intra nasal, which you can buy, or injected subcu, subdermally, like an insulin shot. But if you do this just before sex, it can improve your orgasms and it can cause some warmth and good feelings. It’ll make you feel like you had a good massage or some good foreplay without so much the arousal. If you just inject it subdermally, but you’re not having sex, you’re just reading a book or something, you’ll have some warmth and some good feelings but not necessarily arousal. But if you combine it with sex, it can improve your orgasm. Oxytocin is made by the pituitary gland.
Charles Runels: Growth hormone is another small peptide chain that I’ve actually participated in two different research projects, one lasting several years involving how growth hormone affects the anaerobic threshold or VO2 max in a long term study of Genotropin which was put out by Pharmacia before they sold it to Pfizer. So long story short is I’ve had a chance to look at people who are growth hormone deficient, and what happens when you replace it. The problem with growth hormone, of course, is that it’s been, because of its abuse potential for athletes, it’s been made illegal to write a prescription if you don’t have a good diagnosis, and but yet, there’s controversy about what makes a good diagnosis, so most doctors have become fearful of writing a prescription for growth hormone. But I have seen it affect, not so much libido, but it affects confidence and it helps depression and then indirectly it helps libido.
Charles Runels: The primary thing that of course helps libido is you have luteinizing hormone, follicle stimulating hormone, and these cause the ovaries to make DHEA and testosterone. Okay? So we’ll get to these more later, but just know that luteinizing hormone and follicle stimulating hormone come from the pituitary gland, and if these are really elevated, it means that the person, the woman’s probably going into menopause and this testosterone … It’s absolutely the hormone for arousal, testosterone is, and it’s the hormone when it comes to orgasm. I’ve heard literally hundreds of women tell me that after correcting their testosterone level, their orgasms become much more explosive and powerful and ejaculatory and exciting and bonding with their lover. So testosterone is really huge and we’ll talk more about that later when we talk more about the ovaries.
Charles Runels: But just to mention, this is what controls that when everything’s working normally. The bad news is that if someone’s on birth control pills, it can … It affects, the birth control pills are hormones, right? And so when the pituitary gland sees that, the reason they work as birth control pills is that the pituitary gland thinks there’s enough progesterone or estrogen, and so it decreases the LH and FSH, but as a side effect, testosterone goes down. And it does this in everyone. It’s just that it doesn’t affect everyone.
Charles Runels: But a woman who’s getting migraines, lost libido, weight gain, and depression on birth control pills is probably or at least highly likely and possibly responding to the drop in testosterone levels. So it’s possible that she just insists on being on birth control pills that you could maybe supplement the testosterone and restore her libido and her weight back to normal and help her with migraines and depression. And then when she’s ready to get pregnant, you could just drop both of these. So that’s one strategy that can be done.
Charles Runels: Okay. So all of this is part of the orgasm system. Without testosterone, it’s going to be very difficult to have an orgasm. The other fun thing about testosterone is that the research is really good that you can take it even if you have breast cancer. Now, you’ve got to talk to your doctor about it. Again, I’m not your doctor. But the testosterone down-regulates the estrogen receptors, and some studies show it can actually help protect against recurrence of the breast cancer that can happen and help with the dryness and help with libido, of course. So it’s not necessarily true that you cannot take any hormones just because you had breast cancer.
Charles Runels: Okay. Next, let’s talk about prolactin. Now, prolactin is a bad one. Prolactin is what makes a woman sleepy when she’s breastfeeding. It’s the thing that’s released; it just gushes out when a man has an orgasm or ejaculation, and it’s what makes him sleepy. So if you look at how a man acts right after ejaculating during that refractory period, if you have a prolactin level that’s too high, then you’ll feel like that all the time.
Charles Runels: Doesn’t happen often. I’ll see maybe one or two a year out of several thousand patients, but it does happen. And when you find it, it can be life-changing. It’s usually from a microadenoma, which means that it’s a microscopic secreting gland or tissue within the pituitary gland that does not require surgery. Most people will go on a drug called Dostinex, which they take twice a week, and that blocks the prolactin down and libido returns and energy comes back and they feel like a different person. This can happen in men and women, very simple to find by just doing a blood test. But you want this prolactin level to not be too high. You want it to be normal or it’s going to kill your libido.
Charles Runels: Some books still say you don’t check prolactin level unless something else is goofed up with your pituitary gland. That’s wrong. You just do it on everybody that’s having trouble with their sex. Now, what can happen, if you remember, this is connected to the brain right behind the nose is that if there’s head trauma, even trauma that doesn’t knock someone out, that this pituitary gland can go back and forth and you can have shearing forces there on the pituitary stalk. So one of the things that I have found in my practice, it’s written about, it’s written about in the New England Journal more than once, it’s what often gets diagnosed as post-concussive syndrome or even post-traumatic distress syndrome, is often just the shearing forces on the pituitary stalk cause these hormones to decrease and the person feels tired and depressed and panicky, but what’s really happened is their pituitary gland is not functioning properly, and once you diagnose it and correct everything, things get better.
Charles Runels: Okay, so here’s another interesting thing that happens in the mid-brain. So you’ve got cerebral cortex. You’ve got mid-brain. And then you have this, the base of the brain, and down here where you have fear and … I call it your lizard brain. It’s really interesting that it can cause arousal. For example, if you wanted to have really good sex, you wouldn’t do it, have the sex on the roller coaster or on the motorcycle or in the convertible sports car going fast. But when you have something that causes fear, then that fear causes some things to happen that when it’s over, there becomes arousal.
Charles Runels: So there’s actually some physiology behind the idea of the 50 Shades of Gray, and so if a woman has, if she’s spanked but she’s really not in danger because she’s with her lover who’s just kind of play-spanking her or whatever, then that fear, it’s like being fearful in a scary movie. You really know that you’re sitting in the scary movie and the fear is fun because you know you’re not going to get hurt. So it’s a way to have drama without truly risking danger. And when that happens, whether it’s the fast motorcycle or the roller coaster or the fast sports car, when that fear goes away, there becomes arousal, and that can also be used as part of a way to precipitate orgasm.
Charles Runels: So if you’re at the fair, it would be roller coaster then the sky lift, or the roller coaster and then go home. But it wouldn’t be during the actual fear. It’s after the fear is relieved. So I think with that, I’m going to stop. That’s pretty much the basics of how the brain contributes to the orgasm system, and again, I wanted to keep … I’m basically just laying out and explaining what will eventually go on a chart like this to help put it … My thinking is that, if you can’t draw a picture of it, you don’t understand it. And I’ve tried this.
Charles Runels: I go to meetings, and I’ll lecture at meetings about my O-Shot®, and I’ll find a prominent gynecologist, and just for the fun of it, I’ll say, “Explain to me what happens when a woman has an orgasm.” And I usually get a little mischievous smile and a blank stare. Because it’s, it hasn’t been diagrammed like this. So I don’t claim this to be a static picture we’re going to draw one time and it isn’t added to. I intend to put this in front of other physicians, prominent gynecologists and sex therapists and pelvic floor physical therapists until we have something that feels solid that can go on the wall. So to help us think about how to improve orgasm, the orgasmic response in women.
Charles Runels: Now, having said that, I think we stop for tonight, and next week, we’ll cover how the breasts have feedback systems that have to do with sex, and we’ll go, again, the rest of our course will involve going into how the nervous system works, delivering the different signals, how the … And then the course eventually will end on the clitoral-urethral complex and how the urethra, both the inner and the outer part of the urethra is related to both the corpus cavernosum and the corpus spongiosum is related to the vaginal wall and urethra and how the urethra has a sexual response to it, the anus, and so on.
Charles Runels: So we’ll get to that the last chapter. I think that’s enough for tonight, and then, oh, we’ll also deal with more specific treatments with each part of the anatomy. This will all be recorded, and I’ll put it on the website with a password for you to log in and give me feedback if you don’t want to talk tonight. I’m going to unmute. Got quite a few people on the call, and most people are not willing to talk in front of other people, so if you have a question I’m about to … You can just push the little thing and I’ll answer it. I would love your feedback, and then, I will, again, I’ll send you a free book and with many thanks for helping me basically think more about the content before this becomes a formal book and a chart for doctors’ offices.
Charles Runels: So expect an email from me that goes to this recording and the transcript and a place for you to comment and a password protected membership site so your comments will only be available to other people who have been on the call and to myself as I edit the rest of this book. So does anyone have any questions? If not, then we’ll end the call with this. My intention is that we keep this at about an hour or or less for each chapter.
Charles Runels: Okay. Well, thank you for being on the call, and again, my intention is that, this isn’t just a chart, but it’s a way to think about your sexuality. Hope you picked up some tips that you can use to change your brain chemistry, and if you have, you try some of these ideas this week, again, with your doctor’s permission, obviously I don’t want you manipulating your anti-depressants, but you could go do something that’s safe but gets your pulse up and maybe some of the other things that I talked about. Give me some feedback about hopefully each chapter will give you ideas to make either sexual dysfunction better or your normal sex or your good sex even better.
Charles Runels: I have one last theory and then I’ll shut this down. If you talk to someone, if you just stopped anyone and you say, “Hey, I know a way to increase your VO2max, your anaerobic threshold, and it’s only going to take you 10 minutes and it’s free.” Most people would look at you and say, “I’m not interested.” But if you find someone who’s an elite athlete, they’re going to say, “Yeah, I’m interested. What tips do you have?”
Charles Runels: I think something similar happens with sex. Obviously, you guys are on the call, so you’re interested. But if you talk to someone and you say, “Hey, I have a way to make your good sex even better.” And they say, “Well, I’m not really interested.” In my opinion, what they’re really saying is they don’t want to talk about it. Or their sex is not so good. Because people who are really fit want to know how to be more fit, and people who are having good sex want to know how to make it even better. And so I salute you for being on the call and for having the courage to think about sex and to acknowledge how important it can be to our lives. Bad sex breaks up families and kids wind up living in another state with the other spouse, and it causes remorse and the ripple effect can go through a whole community.
Charles Runels: So sex is so important to our peace of mind, to our families, to our creativity, to our productivity, and even to our spirituality. So I appreciate you being on the call and helping me think about these ideas. I’ll end it with that. Give me some feedback when you get your password to the membership site. Or just shoot me an email with whatever you’re thinking, and I’m very grateful for your participation. Have a good night.
Possible Actions to Discuss with Your Personal Physician
- To make sex better, consider talking about sex with your physician and with a sex/family counselor.
- Good sex evolves out of may different factors relating to health and and that understanding both sex and health can lead to better sex.
- If you’re on a serotonin-uptake inhibitor, ask your physician about ways to counteract its effects on sex.
- Lift weights and go walking (work up to 21 miles a week)
- Have your physician check blood levels of hormones that are important to sex. Recommended…
DIABETES
Glucose
Hemoglobin A1c (Hgb A1c)
Insulin
C-peptideWEIGHT-RELATED
Pancreatic Polypeptide (PP)
Glucagon-Like Polypeptide 1 (GLP-1)
Leptin
ResistinTHYROID
Thyroid Stimulating Hormone (TSH)
Free Thyroxine (Free T4)
Free Triiodothyronine (Free T3)HEMATOLOGY
Complete Blood Count (CBC)
FerritinHORMONES
IGF-1 (to measure growth hormone levels)
Estradiol
Progesterone
DHEA-S
Prolactin
Follicle Stimulating Hormone (FSH)
Luteinizing Hormone (LH)
Sex Hormone Binding Globulin (SHBG)
Testosterone, Total
Testosterone, Bioavailable
CortisolORGAN – LIVER, KIDNEY,
GASTROINTESTINAL
Gastrin
Vitamin B12
Vitamin D 25 OH
Comprehensive Metabolic Panel (CMP)
Blood Urea Nitrogen (BUN)
Creatinine
BUN/Creatinine
Sodium
Potassium
Chloride
Carbon Dioxide
Calcium
Protein, Total
Albumin
Globulin, Calculated
Albumin/Globulin ratio
Bilirubin
Alkaline Phosphatase (ALP)
Aspartate Aminotransferase (AST)
Alanine Aminotransferase (ALT)
References
- Resistance Training to help sex drive
- Sex Matters (Nature)
- Seratonin Up-take Inhibitors decrease sex drive (and strategies to help)
- Aerobic exercise helps orgasm/sex
- Love sickness
- Understanding Women’s Subjective Sexual Arousal Within the Laboratory: Definition, Measurement, and Manipulation
Leave a Reply