The Need for New Treatments for Depression
(Research references for this article are listed at the bottom of the page)
Three hundred million people worldwide suffer the physical and mental pain of depression. And according to the World Health Organization (WHO), depression is the leading cause of disability worldwide. (Whitcup2019)
Everyone has someone close to them who suffered depression to the point that it interfered with life in a significant way. And because a large portion of people does not respond completely to our current therapies, millions of people suffer chronic depression. (Whitcup2019)
In other words, we need something that works better than our current therapies.
Recently, a review article, which covered the past two decades, showed that even though serotonin reuptake inhibitors improve the symptoms of depression for millions of people, they also increased the risk of suicide, and (surprisingly) the article also showed that the whole idea of a “chemical imbalance” of serotonin in the brain causing depression is wrong. (Moncrieff2022) (Wise2022)
If you are currently taking a serotonin reuptake inhibitor (SSRIs), do not stop taking it without the help of your physician--these medications do help many people, and stopping them abruptly can be dangerous.
We now know that depression is not caused by low levels of serotonin!
We need a better way to treat depression.
The Biggest Barrier to Something New & Helpful Entering Your Brain
So many of our present therapies for depression (SSRIs) are based on a debunked theory of serotonin imbalance!
That does not mean that SSRIs are not helping many people, but it does mean that SSRIs are not helping the way we thought they do and it explains why SSRIs do not make chronic depression go a way for millions of people.
For us to keep teaching that depression is caused by a serotonin imbalance is like teaching about the tooth fairy; it ain’t what causes depression.
So, something’s happening when you take SSRIs. What is it?
Here, I’m going to tell you my pure speculation—no research to back it up: SSRIs just dull the senses (more about how later in this note). People feel their depression, they just do not worry about it much. Anorgasmia, continued dysphoria, and an increased risk of suicide and maybe homicide (because you would also be less worried about death)—those are the gifts of SSRIs. Perhaps the depression’s not felt as much, but also fear is not felt as much, which explains why people are less afraid to kill themselves.
So, I am not saying we throw away all antidepressants, but we need to get off the idea that we have depression all figured out and we don’t need something better to treat it; because we do.
Also, as an internist, I would never propose a magic bullet. Depression can also be caused by situations, life events, hypothyroidism, low growth hormone levels, malnutrition, postpartum hormone changes, elevated prolactin from pituitary microadenomas, and much more; Botox would not help any of these.
So, Botox is not a magic bullet to cure all depression. Multiple papers and strong science do suggest that Botox be used for depression as part of a multifactorial approach in some people.
But, BOTOX has not been used as standard therapy for depression partly because we thought we knew that low serotonin was the problem; so how could BOTOX help?
Well, serotonin is NOT the problem, but most doctors still think it is and so think BOTOX for depression does not fit the model—so they do not use it.
In short, the hindrance to knowing something new is not ignorance, it is the illusion that we already know the answers, so we don’t need something new.
We must get over that; we need something better for the treatment of depression, and we need better combination strategies to treat depression.
So, now consider Darwin to consider a new and strong approach that has reached its time.
Darwin & Depression
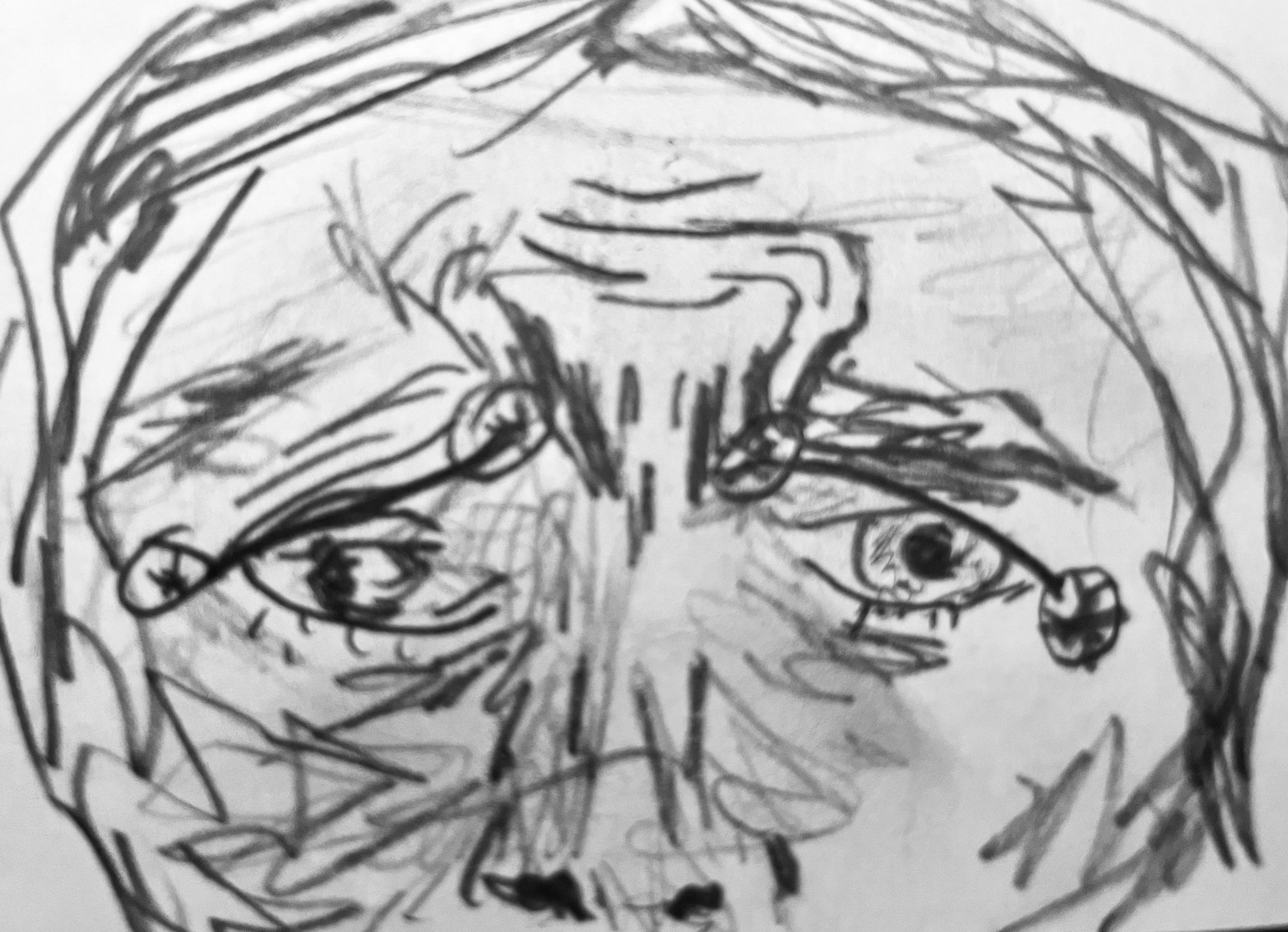
Charles Darwin described muscles that express depression.
First, there is the omega melancholicum which is the combination of the corrugators and the medial part of the frontalis; when someone is worried, anxious, or sad, those emotions create the number 11 signs (from the corrugators), but also this complex of muscles creates a contraction of the medial frontalis, which completes the omega melancholic configuration—it looks like the Greek letter omega.
If you are depressed, you also demonstrate lines called Veraguth’s folds that go from the lateral corner of the eye to the medial eyebrow.
When you draw out the omega and those folds, you see a face that’s worried and sad and tearful and afraid and depressed.
Now that you see the configuration of muscles described by Darwin and others consider how Botox may be of help.
BOTOX and Depression-How it Helps
Multiple studies show that Botox helps depression (see the extensive references in Whitcups excellent textbook chapter 2019).
Even in people that are resistant to antidepressants, BOTOX can help; and now, you know a possible reason why.
And now we know that not only does Botox help depression in those that are resistant to antidepressants, but it also blocks feedback loops that make depression worse. For example, there was one study that showed that if someone says something to you that should be causing you to be sad or depressed, with Botox, there’s a delayed response just in the perception of it. It takes us longer even to think that’s something sad when we hear it.
The Facial Feedback Hypothesis
One of the theories that have been talked about as a possible explanation of how Botox might be helping depression is called the facial feedback hypothesis.
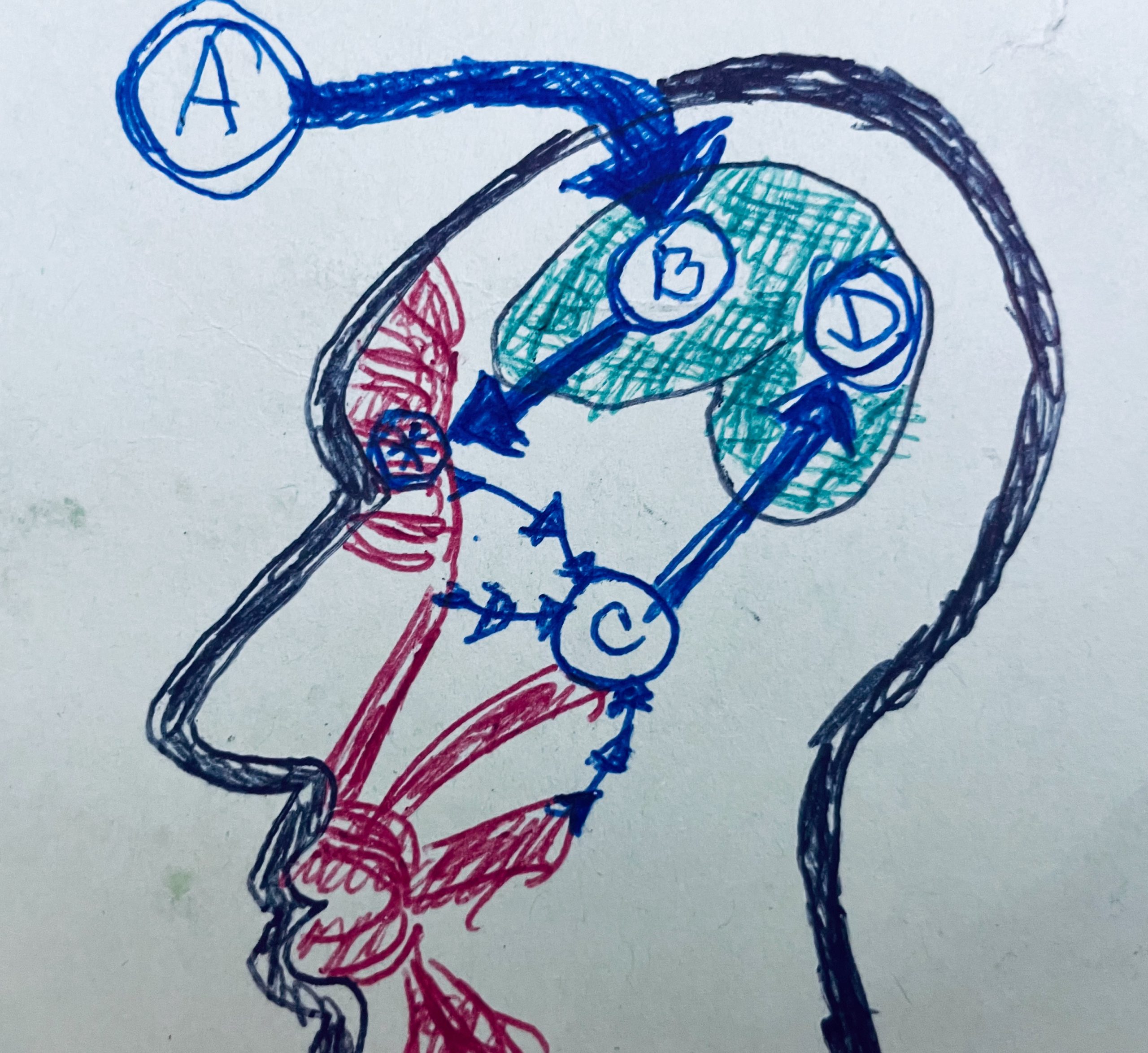
The following diagram shows how it works. (Abdulmohsen2011) (Whitcup2019)
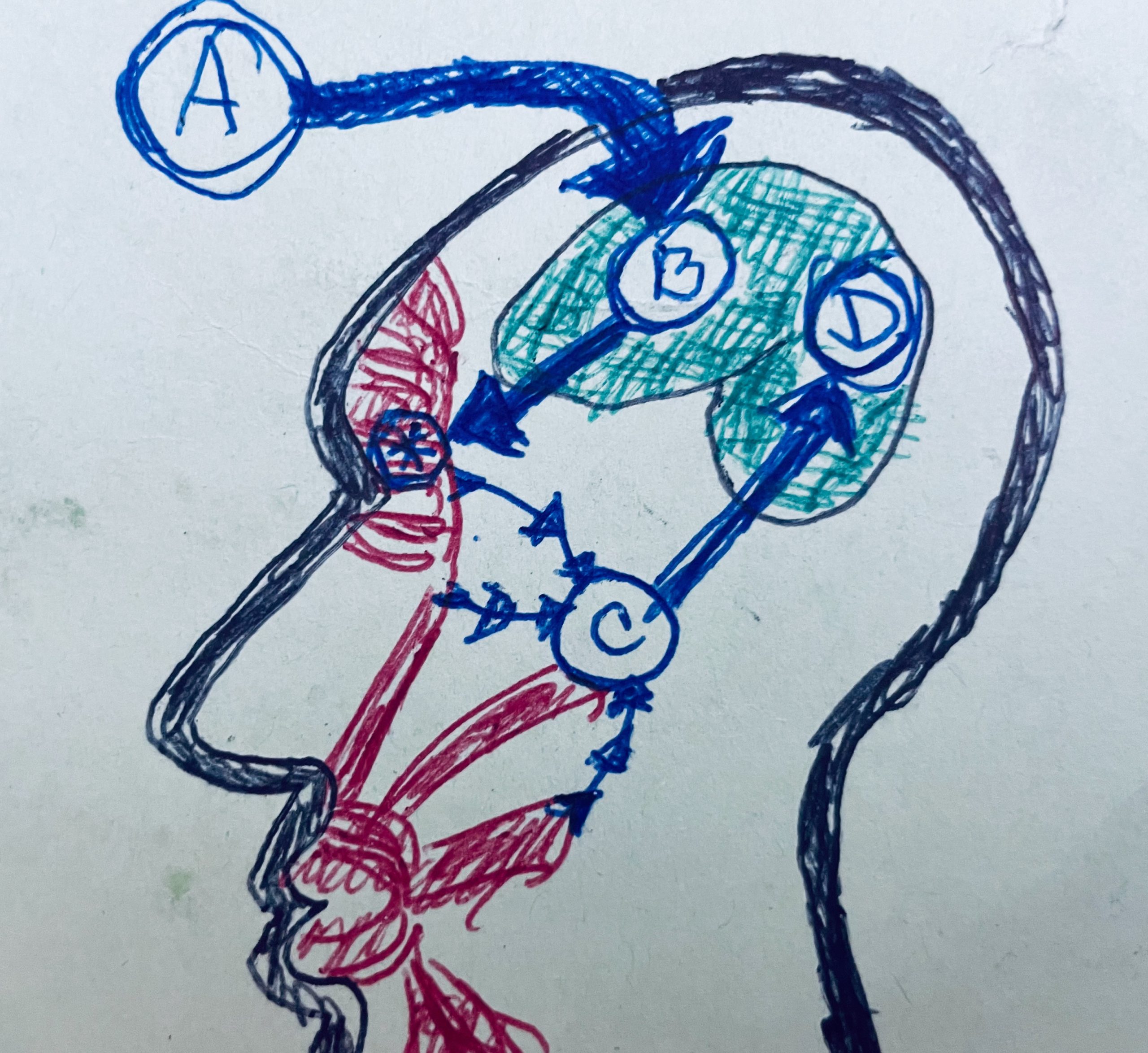
First, you have something coming into consciousness: you hear it, you see it, you think about it; you have this psychological or cognitive information that enters the consciousness and causes what’s called a cold emotion.
So you know about it, but it hasn’t escalated into this visceral thing where you feel like you were punched in the gut—an emotion where you feel heartache, and everybody knows heartache is not a metaphor; your heart aches.
In couples who have been married for over 50 years, the surviving partner bears a death rate after loss of a spouse within a year of the death of their spouse; their heart does not just ache. Their heart breaks, and they fall over dead.
Going from a cold emotion to a warm emotion does not just hurt; it is dangerous. So, stopping the transformation of a cold emotion into a warm emotion is huge (this, in my humble opinion, may also be what SSRIs are doing).
And so (in our diagram of the Facial Feedback Loop), one of the ideas is that once the idea enters the consciousness (illustrated by the “A arrow”), then the “B arrow” perceives it. And it triggers facial musculature activation.
Those muscles that we just described are the main ones that are triggered, the corrugators and the medial part of the frontalis– causing those two configurations, Veraguth’s folds, and the omega melancholicum.
Then the muscles move.
In the diagram of the Facial Feedback Hypothesis, the star with a circle around it illustrates what gets blocked by Botox (the feedback is blocked between C and D).
So the signal to move the muscle just dies, the feedback is blocked, and the emotion stays cold.
But, follow what happens without the Botox: the muscles move, and then C illustrates the proprioception of the movement of the muscles.
So in the musculature, you have nerves that tell the muscles to move.
Then you have nerves that sense that the muscles have been moved. So that’s illustrated by C, the proprioception of the facial muscle signals, the emotional brain, or emotional proprioception.
And then, the emotional proprioception signals enhance the cold emotion and set it on fire into the somatically-enhanced “warm emotion.”
I am not going to keep calling it a warm emotion (as it is called in the medical research). I’m going to call it a pants-on-fire, hot emotion that just burns up your peace of mind.
Think of your peace ignited by C, and then with D, you have not a warm, not a cold emotion like you did with B, but you have D, which becomes a warm emotion or a hot emotion.
Well, guess what happens now?
Facial Feedback Can Cause a Death Spiral
It’s not illustrated in the diagram, but D causes B to tell your muscles to again make the sad face (Omega Melancholicum and Veraguth’s folds)—which goes back to B, which cycles back to D, over and over and over.
Now, you suffer a negative feedback loop that spirals people down—that just can put people collapsed on the floor in tears or vomiting or putting a pistol to their head.
How beautiful is it to have something that blocks that horrific cycle where B does not have the chance to cause that feedback loop?
I am not saying that BOTOX for a grieving widow will make her feel happy. But, BOTOX might attenuate the pain to be bearable and survivable–helping her through the fog to the other side (My observation is that it usually takes a month for every year that someone was married to grieve the loss, in both divorce and death).
Condensed Explanation
When Botox is used in the corrugators, not only do the facial muscles not react to enhance the cold emotions (sadness, anger, and fear) into warm emotions, but also the feedback loop is broken.
IMPORTANT: Because the feedback loop is broken, now there continue to be signals from the face (with Botox use in the corrugators) of calm and happiness–not only blocking the negative feedback but also (by keeping the corrugators relaxed) providing continuing emotional proprioception of peace!
So, the brain may first perceive “sad” (A in the diagram), but C keeps telling the brain, “No, you are not sad, you are at peace; you are calm; you are not afraid; you are not angry.
And that’s what Botox does for you. At least, that is the facial hypothesis.
Speculation…Botox, Depression, & the CNS
Now, what I’m going to tell you is Charles’ hypothesis/speculation about something that would help BOTOX work for depression in ways more than what is implied by the facial feedback hypothesis.
We also know from pain studies (like treating bruxism and migraines) and from animal studies that Botox travels along the axon to the central nervous system and affects this feedback loop centrally.
So, we know there’s also a central effect from BOTOX, not just blocking acetylcholine at the muscle-nerve synapse.
Again, we used to think that Botox is just acting on the acetylcholine receptors so that the nerve cannot stimulate the muscle to contract. But now we know the effects are much more elegant, much more complicated than that. BOTOX helps relieve pain by actually migrating into the spinal column. (Mazzochio2015) (Caleo2018)
So, that means with the treatment of the facial muscles, BOTOX is migrating along the cranial nerves.
So what is that doing?
I have no idea!
But, I cannot imagine that it does nothing–and it could be part of the way BOTOX helps people feel less sad.
But, even though we do not know for sure how BOTXO helps depression, we do know (from multiple studies) that some people who suffer from depression so severe they do not respond to medications are helped by treating the corrugators with BOTOX.
And, we know that their depression is not caused by a paucity of serotonin.
What About Insurance?
So, what the heck are we waiting for?
In my opinion, we should be offering Botox to everyone who is clinically sad and not responding to non-pharmacological measures (I still think 21 miles a week on foot is one of the best treatments for depression). And we now know that BOTOX can help some people who suffer from personality disorders.
It becomes almost an ethical problem to not use BOTOX for depression (assuming none of the contraindications like pregnancy and myasthenia gravis).
So, what keeps us from offering BOTOX for depression?
You might say, “Insurance is not paying for BOTOX for depression.”
I would say, “Whatever!?”
We are talking about a treatment that costs much less than a new set of tires. This is something that’s like buying a night in a hotel room every three months or, these days, filling your car with gas two or three times.
Not a Magic Bullet
First, just to repeat, I am at heart an internist; in no way do I think BOTOX is a magic bullet to cure everyone’s depression. All you know about the need for healthy living, treating addiction, the need for counseling, the need for good medical diagnosis–all of that and more still applies.
What I am saying is that (especially with the recent debunking of the serotonin “chemical imbalance” theory of depression), we do need more combination therapies and that BOTOX (because it is effective and safe) should be a commonly used tool to help those suffering the ravages of depression.
If you could be pregnant or if you have myasthenia gravis, you should not get BOTOX. Otherwise, I know of few therapies that have the potential for as much good with such a strong safety profile.
Thankfully, the same techniques that help people look better also help them feel better. So, when I do your BOTOX, I will be doing the very same thing I do when I treat frown lines (or the number 11’s).
My Request
If you think you would like to try BOTOX to help with your depression, DO NOT STOP TAKING ANY ANTIDEPRESSANTS YOU MAY BE TAKING; you can take your antidepressants and still use BOTOX to help them work better. Or, if you suffer a milder depression or anxiety (not on medications and not contemplating suicide) and want to see if BOTOX might help you feel better, then that is also good.
Here’s where to make an appointment with me<–
Best regards,

Charles Runels, MD
References
The fact that botox has been shown to improve depression an ALL treatment areas (including upper and lower limb spasticity and blepharospasm) argues more towards the central migration theory. And the amount of improvement of depression in all treatments areas is about the same, meaning that it’s not completely dose dependent.